When working with patients in a deep coma, doctors interpret a flat EEG reading as a sign that the person is brain-dead and with little chance of waking up. But a new Canadian study raises the possibility of ongoing brain activity beneath that flat line.
The observation of this never-before-detected brain activity, which the University of Montreal researchers are calling Nu-complexes, poses challenging questions about the definition of brain death and how to handle the moment when flatlining occurs. Just as importantly, the observation is questioning the efficacy of using EEG flatlines as the ultimate sign of brain death; some scientists are suggesting that we should now abandon the idea that a flat EEG proves zero neuronal activity.
https://gizmodo.com/the-meaning-of-death-how-do-we-know-someone-is-no-long-5915339
The researchers, a team led by Florin Amzica, were tipped off to this possibility after observing a human patient in a deep hypoxic coma who was placed under a powerful anti-epileptic medication on account of health issues. His doctor, Bogdan Florea, observed unexplainable phenomena — tiny intermittent bursts of activity that were interrupting an otherwise flatline signal and lasting for a few seconds.
https://gizmodo.com/the-neuroscience-of-comas-or-what-it-means-to-be-trapp-5966630
Given the possibility of cerebral activity, Florea asked Amzica to investigate further.
Intrigued, the Montreal team decided to simulate the coma in cats. They did so by administering the anesthetic isoflurane, which puts the cats into a deep, but completely reversible, coma (the standard animal model for neurological studies).
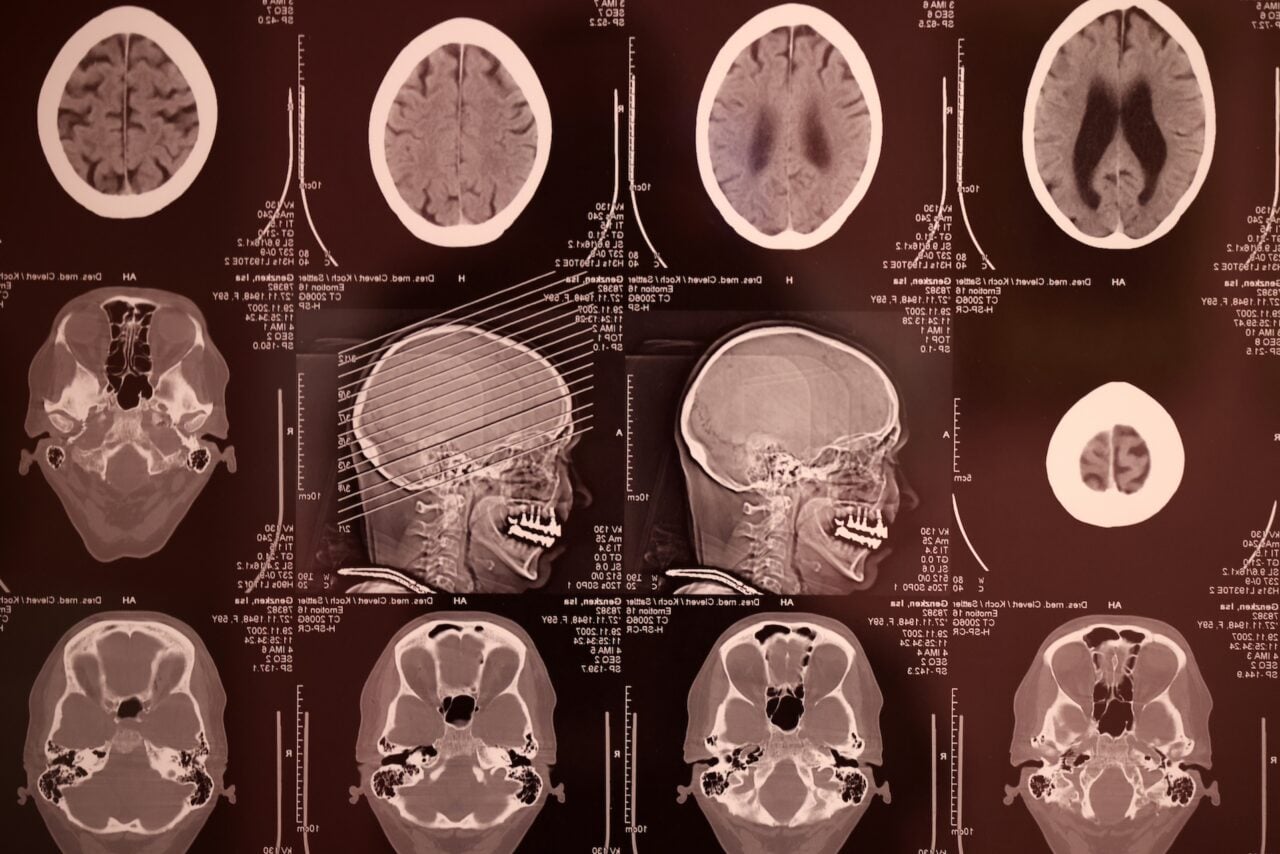
In this state, the researchers used deep-brain electrodes to observe cerebral activity in the cats placed in the coma. Specifically, they measured oscillations generated in the hippocampus, the part of the brain responsible for learning processes and memory. These oscillations, now dubbed Nu-complexes, were transmitted to the brain’s cerebral cortex — the brain’s master control.
At the same time, traditional EEG recordings showed a flatline.
Cortical and hippocampal neuronal activity during comatose state. Credit: Amzica et al.
In a release, Amzica noted the implications and added a word of caution:
Those who have decided to or have to ‘unplug’ a near-brain-dead relative needn’t worry or doubt their doctor. The current criteria for diagnosing brain death are extremely stringent. Our finding may perhaps in the long term lead to a redefinition of the criteria, but we are far from that. Moreover, this is not the most important or useful aspect of our study.
What he’s talking about is the therapeutic potential — the neuroprotection — of extreme deep comas. In other words, it’s possible that this is the brain’s way of preventing a kind of atrophy when in such a state.
Read the entire study at PLoS One: “Human Brain Activity Patterns beyond the Isoelectric Line of Extreme Deep Coma.”